

 Medical, Dental & Pharmacy
Medical, Dental & Pharmacy
- Medical
- Ambulatory Surgical Services
- Children's Services
- Chiropractic
- Clinic Services
- Community First Services and Supports (CFSS)
- Early Intensive Development and Behavioral Intervention (EIDBI)
- Equipment and Supplies
- HCBS
- Hearing Services
- Home Care Services
- Hospice Services
- Hospital Services
- Housing Stabilization Services
- Immunizations and Vaccinations
- Laboratory/Pathology, Radiology, and Diagnostic Services
- Language Interpreter Services
- Long-Term Care
- Medication Reconciliation
- Mental Health Services
- Optical Services
- Personal Care Assistance (PCA) Services
- Physician and Professional Services
- Recuperative Care
- Rehabilitation Services
- Renal Dialysis
- Restricted Recipient Program
- School-Based Community Services
- Substance Use Disorder
- Telehealth Services
- Transportation
- Tribal and Federal Indian Health Services
- Dental
- Pharmacy
Covered Services
The purpose of the dental program is to provide for the medically necessary oral health needs of the member and to maintain an appropriate level of dental health according to dental community standards.
Refer to the following covered services for specific current coverage:
- Alveoloplasty/Gingivectomy
- Anesthesia
- Fluoride Varnish Application (FVA)
- Sleep Apnea Appliance
- Teledentistry
- Temporomandibular Joint Disorder (TMD)
PrimeWest Health considers dental services provided beyond those identified as covered and in excess of the frequencies noted as non-covered services and the member’s responsibility. Providers must inform the member before providing a non-covered service for which the member is financially responsible.
PrimeWest Health covers dental services that are medically necessary for covered members.
This list of covered services is not all-inclusive.
Diagnostic
- Oral evaluations – must consist of a face-to-face visit with a dentist
- D0120 – Periodic oral evaluation
- Limited to twice per year
- Cannot be performed on same date as a limited or comprehensive evaluation
- D0140 – Limited oral evaluation
- Limited to once per day
- Cannot be performed on same date as a periodic or comprehensive oral evaluation
- Documentation must include notation of the specific oral health problem or complaint
- D0145 – Oral evaluation for a patient under age 3
- Cannot be performed on same date as D1330
- D0150 – Comprehensive oral evaluation
- Once every two years
- Cannot be performed on same date as a periodic or limited evaluation
- D0120 – Periodic oral evaluation
- Dental X-rays
- D0210 – Covered once every 2 years in an office setting or as needed in the operating room or ambulatory surgical center.
- D0220 – D0230 Periapical X-rays
- Four per date of service (does not include intraoral complete series)
- D0270 – D0277 – Bitewing X-rays, one series per calendar year
- D0330 – Once per 5 years beginning January 1, 2010, except:
- With a scheduled outpatient facility or freestanding ASC procedure (include claim attachment identifying hospital/ASC name)
- For a medically necessary diagnosis and follow-up of oral and maxillofacial pathology and trauma (include claim attachment with a description of the pathology or trauma and the medical diagnosis identified)
- Once every 2 years for patients who cannot cooperate for intraoral film due to a developmental disability or medical condition that does not allow for intraoral film placement (include claim attachment identifying developmental disability or medical condition that does not allow for intraoral film placement)
- D0340 – Limited to one cephalometric film per every five years
- D0364 – D0384 – Cone Beam Computed Tomography (CBCT).
- D0372 – Once every two years
- D0396 – 3D printing of a 3D dental surface scan
Preventive
- Dental prophylaxis
- D1110 – prophylaxis – adult, twice per calendar year, up to two additional if medically necessary
- D1120 – prophylaxis – child, twice per calendar year, up to two additional if medically necessary
- Fluoride treatment and varnish application
- Topical application of fluoride varnish (D1206) once per six months
- Topical application of fluoride (excluding varnish) (D1208) once per six months
- D1206, D1208, and D9910 cannot be performed on same date
- D1354 – Interim caries arresting medicament application – per tooth
- D1355 – Caries preventative medicament application – per tooth
- D1330 – Oral Hygiene Instruction
- Oral hygiene instruction is considered an ongoing integral component of every dental visit.
- PrimeWest Health reimburses oral hygiene instructions once per year.
- Document the amount of time above and beyond the standard prophylaxis, gross debridement, scaling and root planing, or other scheduled service that was required for oral hygiene instruction.
- MN Rules part 9505.0270, subp. 1. E. defines oral hygiene instruction as an organized education program carried out by or under the supervision of a dentist to instruct a patient about the care of the patient’s teeth.
- A copy of the organized educational program must be retained in the patient chart and include the following:
- Assessment findings/risk factors for oral disease specific to the patient
- Detailed counseling components presented, based on the assessments/risk factors
- Objectives of the customized care plan
- Educational methodology used and how each educational component was presented
- The amount of time scheduled to complete the organized education program
- For children under age six years, the name of the parent/legal guardian to whom the educational program was presented
- Any additional oral hygiene instruction services must meet the specifications of utilization criteria.
- D1351 – Sealants
- Once per tooth, per five years, per permanent molar (tooth numbers 1 – 3, 14 – 16, 17 – 19, and 30 – 32)
- Space maintainers
- D2991 – Application of hydroxyapatite regeneration medicament, per tooth
Restorative
- D2140 – D2161, D2330 – D2394: Amalgam and composite fillings
- Limited to once in 90 days for the same tooth
- Posterior fillings are all reimbursed at the amalgam rate
- PrimeWest Health prohibits balance billing posterior composites to the member
- Laboratory resin crowns that meet the specifications of utilization review
- Prefabricated stainless steel or prefabricated resin crowns
- Sedative fillings
- Cannot be performed on same date as D9110
Endodontics
- D3310 – D3330: Once per tooth per lifetime.
- D3346 – D3348: Retreatment of a previous root canal
- D3355 – Initial visit of a pulpal regeneration procedure
- D3356 – Interim medication replacement for pulpal regeneration
- D3357 – Completion of treatment
Periodontics
PrimeWest Health encourages providers to utilize the American Academy of Periodontology's (AAP) Three Steps to Staging and Grading a Patient:
- Initial case overview to asses disease
- Establish state
- Establish grade. The AAP guidelines for staging and grading should be used to classify the severity and extent of a member’s periodontal disease and to provide an indicator of the rate of progression of their disease.
- D4322: Splint – Intra-Coronal; Natural Teeth or Prosthetic Crowns (once per calendar year)
- D4323: Splint – Entra-Coronal; Natural Teeth or Prosthetic Crowns (once per calendar year)
- D4341 – D4342: Scaling and root planing that meets the specifications of utilization criteria
- D4910: Periodontal maintenance (up to four per calendar year following the completion of D4341 or D4342)
- After 24 months, D4910 is not payable unless D4341 or D4342 is performed again under a new Service Authorization
- D4355: Full mouth debridement – once every two years
Oral cavity indicators must only be used for periodontal services to designate the quadrants where the service was or will be provided. Bill using the appropriate numeric oral cavity designation code: 10, 20, 30, or 40.
Prosthodontics
- Removable full dentures
- Removable partial dentures that meet the specifications of utilization criteria
- Reline, repair, or rebase of a removable complete or partial denture
- Fixed bridges/dental implant related services that meet the specifications of utilization criteria
- Porcelain/metal crowns in conjunction with a medically necessary fixed bridge/implant that meet the specifications of utilization criteria.
- Current Dental Terminology (CDT) codes: D6092 (Recement implant/abutment supported crown) and D6093 (Recement implant/abutment supported fixed partial denture) do not require authorization but are subject to utilization review. All other dental implants codes require authorization.
Removable Dentures – Complete and Partial
Initial placement or replacement of a removable prosthesis is limited to once every three years per member unless one (or more) of these conditions apply:
- Replacement of a removable prosthesis in excess of this limit is eligible for payment if the replacement is necessary because the removable prosthesis was misplaced, stolen, or damaged due to circumstances beyond the member’s control. When applicable, the member’s degree of physical and mental impairment must be considered in determining whether the circumstances were beyond a member’s control. Submit a completed Denture Replacement Request Form along with the Service Authorization.
- Replacement of a partial prosthesis is eligible for payment if the existing prosthesis cannot be modified or altered to meet the member’s dental needs.
- Service for a removable prosthesis must include instruction in the use and care of the prosthesis and any adjustment necessary to achieve a proper fit during the six months immediately following the provision of the prosthesis. Document the instruction and the necessary adjustments, if any, in the member’s dental record.
- A partial denture with metal-based framework requested on an authorization may be downgraded to a resin-based appliance because the criteria are not met. The provider could still choose to provide the metal-based removable prosthesis, but will only be reimbursed by PrimeWest Health for the resin-based partial. The claim should reflect the actual appliance provided. Chart documentation must reflect this.
- Bill denture identification (ID) only for dentures previously made without ID markers. Denture identification for new dentures or partials will deny.
- Replacement of missing or broken teeth allows for a maximum number of five teeth.
Undeliverable Removable Prostheses
PrimeWest Health pays a percentage payment of the scheduled allowable for undeliverable removable prostheses. Submit an attachment for the claim documenting the following:
- Reason for non-delivery noted in the patient chart
- Explanation that includes the incurred lab charges and the percent of work completed
Fax the required documentation by the end of the next business day after submitting the electronic claim. The completed prosthesis must be kept in the provider’s office, in a deliverable condition, for a period of at least two years.
Payment will be prorated based on the percentage completed and utilization review.
Other Services
- D7280 – Surgical access of an unerupted tooth
- D7283 – Placement of device to facilitate eruption of impacted tooth
- D7510 – Incise and drain
- D9110 – Palliative care for the relief of pain
- D9222 – D9248
- Deep sedation/general anesthesia
- Intravenous (IV) conscious sedation/analgesia
- Nitrous oxide analgesia, anxiolysis
- Regardless of the age of the child, the determination of medical necessity for general anesthesia in conjunction with dental services must consider the information related to general anesthesia established under the “Guideline on Behavior Guidance for the Pediatric Dental Patient” by the American Academy of Pediatric Dentistry and the American Dental Society of Anesthesiology.
- Intravenous moderate (conscious) sedation/analgesia and non-intravenous conscious sedation do not require a prior authorization if the covered dental service cannot be performed safely without it or would otherwise require the service to be performed under general anesthesia in a hospital or surgical center
- D9410 – House/extended care facility call
- Services performed in a school or Head Start program are considered house calls; can only be billed for on-sight delivery of covered services. Use Place of Service (POS) code 03.
- Extended care facilities are long-term care facilities (LTCFs). These include the following: nursing facilities (NFs), Skilled Nursing Facilities (SNFs), boarding care homes (BCHs), Institutions for Mental Disease (IMDs), Intermediate Care Facilities for the Developmentally Disabled (ICF/DDs), hospices, Minnesota Extended Treatment Options (METO), and Swing Beds (an NF bed in a hospital).
- It must be billed in combination with a separate code that indicates the covered service provided. Effective July 1, 2016, D9410 can be billed with D5992 for fitting of a removable prosthesis up to five times per year for non-pregnant adults. D5992 is an informational code and will be paid at $0.
- D9920 – Behavior management that is documented as a service necessary to ensure that a covered dental procedure is correctly and safely performed
- D9610, D9612 – Therapeutic parenteral drugs
- D9952 – Occlusal adjustment, limited
- Once per day
- Includes only those services defined by the most current edition of the CDT
- D9956 – Administration of home sleep apnea test
- D9957 – Screening for sleep-related breathing disorders
- Drugs (D9610, D9612, and D9630)
- Additional information must be entered in the notes section of the 837D
- Name of drug
- National Drug Code (NDC) of drug
- Dosage
- Additional information must be entered in the notes section of the 837D
Authorization Requirements
Unnecessary authorizations are costly. Routine services do not require authorization. The following dental services require Service Authorization by PrimeWest Health. When submitting dental X-rays with a Service Authorization request, X-rays must be labeled with the member's name and date of the X-rays.
Unspecified Diagnostic Procedure
Provide information regarding what testing you would like to do and the reasoning for it. If this code is used for BSS, then Service Authorization is not needed.
Oral Hygiene Instruction
D1330 – Oral hygiene instructions
Authorization is required after the service has been provided once for the member. Ambulatory Surgical Centers (ASC), Outpatient Hospital Ambulatory Payment Classification (APC) Payments, and Critical Access Hospitals (CAH) are exempt from prior authorization requirements.
For authorization, submit a copy of the organized education program to be carried out by or under the supervision of the dentist to instruct the patient about the care of their teeth.
Requests for authorization must include the following:
- Assessment findings/risk factors for oral disease specific to the patient
- Detailed counseling components presented, based on the assessments/risk factors
- Objectives of the customized care plan
- Educational methodology used and how each educational component is to be presented
- The amount of time scheduled to complete the organized education program
- For children under age 6 years, the name of the parent/legal guardian to whom the educational program is to be presented
Periodontal Services
PrimeWest Health encourages providers to utilize the American Academy of Periodontology's (AAP) Three Steps to Staging and Grading a Patient:
- Initial case overview to asses disease
- Establish state
- Establish grade. The AAP guidelines for staging and grading should be used to classify the severity and extent of a member’s periodontal disease and to provide an indicator of the rate of progression of their disease.
Authorization is always required.
Requests for authorization for periodontal services must be submitted with the following dental history, case information, and documentation:
- Current radiographs; panoramic, full mouth series or bitewing
- Chart documentation including:
- Periodontal Scaling and Root Planing (SRP) Service Authorization Request Supplemental Document
- Current periodontal charting with notations of :
- Six point measurements
- For periodontal scaling and root planing – pocket depths must be greater than four millimeters
- Mobility
- Presence of pathology
- Periodontal prognosis
Classification of the periodontology case type which must be in accordance with documentation established by the AAP.
- D4210 – Gingivectomy or gingivoplasty – per quadrant
- D4211 – Gingivectomy or gingivoplasty – per tooth
- D4240 – Gingival flap procedures, including root planning – per quadrant
- D4241 – Gingival flap procedure, including root planing – one to three contiguous teeth
- D4245 – Apically positioned flap
- D4249 – Crown lengthening – hard and soft tissue, by report
- D4260 – Osseous surgery, including flap entry and closure per quadrant
- D4261 – Osseous surgery (including flap entry and closure) – one to three teeth, per quadrant
- D4263 – Bone replacement graft – first site in quadrant
- D4264 – Bone replacement graft – each additional site in quadrant
- D4266 – Guided tissue regeneration – resorbable barrier, per site, per tooth
- D4267 – Guided tissue regeneration – non-resorbable barrier, per site, per tooth (includes membrane removal)
- D4268 – Surgical revision procedure, per tooth
- D4270 – Pedicle soft tissue grafts
- D4271 – Free soft tissue grafts including donor site
- D4273 – Subepithelial connective tissue graft procedure (including donor site surgery)
- D4274 – Distal or proximal wedge procedure (when not performed in conjunction with surgical
- D4275 – Soft tissue allograft
- D4276 – Combined connective tissue and double pedicle graft, per tooth
- D4341* – Periodontal scaling and root planing – four or more teeth per quadrant
- D4342* – Periodontal scaling and root planing – one to three teeth per quadrant
- D4381 – Localized delivery of chemotherapeutic agents via a controlled release vehicle into diseased crevicular tissue, by tooth, by report
- D4910 – Periodontal maintenance
- After 24 months, D4910 is not payable unless D4341 or D4342 is performed again under a new Service Authorization
- D4999 – Unspecified periodontal procedure
*D4341 and D4342 do not require Service Authorization when performed in outpatient hospital or freestanding ASC.
Crowns
Authorization requests for crowns must meet all of the following criteria:
- Dentition must have a good long-term prognosis and minimal mobility.
- Pocket depth of 6 mm or less.
Authorization requests must include medical and dental history that supports medical necessity, copies of current radiographs that show the current dental condition, and a complete treatment plan and long-range prognosis for the remaining dentition.
Note: For codes D2740 – D2794, evidence that a root canal has been performed must also be submitted with the authorization request.
- D2720 – Crown, resin with high noble metal
- D2721 – Crown, resin with predominantly base metal
- D2722 – Crown, resin with noble metal
- D2950 – Core buildup
- D2952 – Post and core, in addition to crown
- D2953 – Each additional indirectly fabricated post-same tooth
- D2960 – Labial veneer-(laminate) chairside
- D2961 – Labial veneer-(resin laminate) laboratory
- D2962 – Labial veneer-(porcelain laminate) laboratory
- D2971 – Additional procedures to construct crown
- D2975 – Coping
- D2999 – Unspecified restorative procedure, by report
Endodontics
Authorization always required for the following codes and requests for endodontic treatment must meet all of the following criteria:
- D3460 – Endodontic endosseous implant
- D3999 – Unspecified endodontic procedure, by report
- Dentition must have a good long-term prognosis and minimal mobility.
- Pocket depth of 6 mm or less.
Submit requests for authorization with the following dental history, case information, and documentation:
- Medical and dental history that supports the medical necessity.
- Copies of current radiographs that show the current dental condition.
- Complete treatment plan and long-range prognosis for the remaining dentition.
Complete Dentures
Authorization required only if replacement is performed in less than three years.
If requesting replacement of existing prosthesis:
- Include the specific reason for request
- Specify why existing full or partial denture cannot be relined, rebased, or repaired
- Submit a completed Denture Replacement Request Form if replacement is needed due to circumstances beyond member’s control
Complete Overdenture
Authorization is always required.
Partial Dentures
Authorization is always required.
Initial placement or replacement of a removable prosthesis is limited to once every three years.
Requests for authorization for partial dentures, interim or permanent, must be submitted with the following dental history, case information, and documentation:
- History regarding all previous prostheses
- Dental history pertinent to request
- Diagnostic radiographs of the current dental condition for all remaining teeth of the involved arch. Include copies (not originals) of X-rays. Submit a panoramic image to show bone levels of the remaining abutment teeth.
- Indicate on the American Dental Association (ADA) claim form all missing teeth and teeth to be replaced by the partial denture
- “X” all missing teeth
- Identify all teeth to be replaced by partial dentures
- Current six point periodontal charting and periodontal prognosis of remaining teeth.
PrimeWest Health will approve a removable partial denture (RPD) if the following conditions are met:
- The patient is missing an anterior tooth and radiographs demonstrate adequate space for replacement of the missing anterior tooth or either of the following:
- The patient has fewer than 10 posterior teeth in occlusion (unless the remaining teeth are not periodontally sound)
- The RPD is required to stabilize occlusion by minimizing the tipping or extrusion of existing teeth (depending upon age and existing situation reflected in the clinical notes and X-rays).
- An RPD opposing a complete denture will be allowed to provide balancing occlusion. Balancing occlusion is lacking when five posterior teeth are missing in one arch, not including third molars.
- For immediate RPDs, provide the following additional information, if applicable:
- Date previous denture was placed, if there was one
- Identification of teeth now being extracted and those being replaced
- Explanation as to why extracted teeth cannot be added to current RPD
Requests for cast metal removable prosthesis must meet all of the following criteria:
- The crown to root ratio must be at or better than 1:1 for abutment teeth
- The surrounding abutment teeth and the remaining teeth must not have extensive decay or extensive periodontal disease; and
- The abutment teeth must not have large restorations or stainless steel crowns
If requesting replacement of existing prosthesis:
- Include the specific reason for request
- Specify why existing full or partial denture cannot be relined, rebased, or repaired
- Submit a completed Denture Replacement Request Form if replacement is needed due to circumstances beyond member’s control
Codes
- D5211 – Upper partial – resin base (including any conventional clasps, rests, and teeth)
- D5212 – Lower partial – resin base (including any conventional clasps, rests, and teeth)
- D5213 – Upper partial – cast metal base with resin saddles (including any conventional clasps, rests, and teeth)
- D5214 – Lower partial – cast metal base with resin saddles (including any conventional clasps, rests, and teeth)
- D5221 – Immediate maxillary partial denture – resin base (including any conventional clasps, rests, and teeth)
- D5222 – Immediate mandibular partial denture – resin base (including any conventional clasps, rests, and teeth)
- D5223 – Immediate maxillary partial denture – cast metal framework with resin denture bases (including any conventional clasps, rests, and teeth)
- D5224 – Immediate mandibular partial denture – cast metal framework with resin denture bases (including any conventional clasps, rests, and teeth)
- D5225 – Maxillary partial denture – flexible base (including any clasps, rests, and teeth)
- D5226 – Mandibular partial denture – flexible base (including any clasps, rests, and teeth)
- D5820 – Interim Partial Denture – upper (Maxillary)
- D5821 – Interim Partial Denture – lower (Mandibular)
- D5862 – Precision attachment, by report
- D5864 – Overdenture – partial maxillary
- D5866 – Overdenture – partial mandibular
- D5867 – Replacement of semi-precision or precision attachment
- D5875 – Modification of removable prosthesis
- D5899 – Unspecified removable prosthodontic procedure
- D5911 – Facial moulage (sectional)
- D5912 – Facial moulage (complete)
- D5937 – Trismus appliance
- D5951 – Feeding aid
- D5952 – Speech aid prosthesis, pediatric
- D5953 – Speech aid prosthesis, adult
- D5954 – Palatal augmentation prosthesis
- D5958 – Palatal lift prosthesis, interim
- D5959 – Palatal lift prosthesis, modification
- D5960 – Speech aid prosthesis, modification
- D5982 – Surgical stent
- D5983 – Radiation carrier
- D5984 – Radiation shield
- D5985 – Radiation cone locator
- D5986 – Fluoride gel carrier
- D5987 – Commissure splint
- D5992 – Adjust maxillofacial prosthetic appliance, by report. Informational-only code; can be billed in conjunction with D9410 a maximum of five times per calendar year. Will pay at $0.
Dental Implant Related Services
A complete treatment plan, including prosthesis and all related services, must be approved prior to the start of treatment. Specific syndromes or conditions do not pre-qualify a member for implant approval.
Requests for dental implants must meet all of the following criteria:
- Bone and tooth loss that compromises chewing or breathing
- The implants must be medically necessary and cost-effective
Submit requests for authorization with the following documentation:
- Medical, dental, and behavioral histories that support medical necessity for the member
- Additional pertinent information
- Member's mental or physical condition, including ICD-CM and DSM-5 diagnoses when pertinent, that causes their inability to use a removable denture
- An explanation of the reason the member is unable to use a conventional removable denture
- Copies of current diagnostic imaging that demonstrate the current dental or oral condition
- The specific treatment plan and the long-range prognosis for the remaining dentition (if any)
- Current six-point periodontal charting including clinical attachment loss and mobility per tooth when relevant
Authorization is always required for the following dental implant-related codes. Only the codes listed below can be submitted for authorization.
Codes
- D6010 – Surgical placement of implant body: endosteal implant
- D6011 – Surgical access to an implant body (second stage implant surgery)
- D6012 – Surgical placement of interim implant body for transitional prosthesis: endosteal implant
- D6013 – Surgical placement of mini-implant
- D6040 – Surgical placement: eposteal implant
- D6050 – Surgical placement: transosteal implant
- D6055 – Implant connecting bar
- D6056 – Prefabricated abutment
- D6057 – Custom abutment
- D6058 – Abutment supported porcelain/ceramic crown
- D6059 – Abutment supported porcelain fused to metal crown (high noble metal)
- D6060 – Abutment supported porcelain fused to metal crown (predominantly base metal)
- D6061 – Abutment supported porcelain fused to metal crown (noble metal)
- D6062 – Abutment supported cast metal crown (high noble)
- D6063 – Abutment supported cast metal crown (predominately base metal)
- D6064 – Abutment supported cast metal crown (noble metal)
- D6065 – Implant supported porcelain/ceramic crown
- D6066 – Implant supported porcelain fused to metal crown
- D6067 – Implant supported metal crown
- D6068 – Abutment supported retainer for porcelain/ceramic fixed partial denture (FPD)
- D6069 – Abutment supported retainer for porcelain fused to metal FPD (high noble metal)
- D6070 – Abutment supported retainer for porcelain fused to metal FPD (predominately base metal)
- D6071 – Abutment supported retainer for porcelain fused to metal FPD (noble metal)
- D6072 – Abutment supported retainer for cast metal FPD (high noble metal)
- D6073 – Abutment supported retainer for cast metal FPD (predominately base metal)
- D6074 – Abutment supported retainer for cast metal FPD (noble metal)
- D6075 – Implant supported retainer for ceramic FPD
- D6076 – Implant supported retainer for porcelain fused to metal FPD
- D6077 – Implant supported retainer-forecast metal FPD (titanium, titanium alloy, or high noble metal)
- D6080 – Implant maintenance procedures, including: removal of prosthesis, cleansing of prosthesis, and abutment reinsertion of prosthesis
- D6082 – Implant supported crown – porcelain fused to predominantly base alloys
- D6083 – Implant supported crown – porcelain fused to noble alloys
- D6084 – Implant supported crown – porcelain fused to titanium and titanium alloys
- D6086 – Implant supported crown – predominantly base alloys
- D6087 – Implant supported crown – noble alloys
- D6088 – Implant supported crown – titanium and titanium alloys
- D6094 – Abutment Supported Crown (Titanium)
- D6097 – Abutment supported crown – porcelain fused to titanium and titanium alloys
- D6098 – Implant supported retainer – porcelain fused to predominantly base alloys
- D6099 – Implant supported retainer for FPD – porcelain fused to noble alloys
- D6120 – Implant supported retainer – porcelain fused titanium and titanium alloys
- D6121 – Implant supported retainer for metal FPD – predominantly base alloys
- D6122 – Implant supported retainer for metal FPD – noble alloys
- D6123 – Implant supported retainer for metal FPD – titanium and titanium alloys
- D6190 – Radiographic/Surgical Implant Index
- D6194 – Abutment Supported Retainer Crown For FPD (Titanium)
- D6195 – Abutment supported retainer – porcelain fused to titanium and titanium alloys
Fixed Partial Denture (FPD) – Pontics
Authorization is required for fixed dentures (that are cost-effective) for people who are unable to use removable dentures because of their medical condition.
Replacement of damaged fixed denture for individuals who are unable to use a removable denture due to a medical condition requires authorization.
Requests for authorization for fixed denture must be submitted with the following documentation:
- Medical and dental history that supports the medical necessity
- The member’s mental/physical condition, including International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) and Diagnostic and Statistical Manual of Mental Disorders (DSM-5) diagnoses that cause the member’s inability to use a removable denture
- An explanation of the reason the member is unable to use a removable denture
- Radiographs of the current dental condition. Include copies (not originals) of X-rays.
- The specific treatment plan and the long-range prognosis for the remaining dentition
Codes
- D6205 – Pontic – indirect resin-based composite
- D6210 – Pontic – cast high noble metal
- D6211 – Pontic – cast predominantly base metal
- D6212 – Pontic – cast noble metal
- D6214 – Pontic – titanium
- D6240 – Pontic – porcelain fused to high noble metal
- D6241 – Pontic – porcelain fused to predominantly base metal
- D6242 – Pontic – porcelain fused to noble metal
- D6243 – Pontic – porcelain fused to titanium and titanium alloys
- D6245 – Pontic – porcelain/ceramic
- D6250 – Pontic – resin with high noble metal
- D6251 – Pontic – resin with predominantly base metal
- D6252 – Pontic – resin with noble metal
- D6253 – Pontic – provisional
Fixed Partial Denture (FPD) Retainers – Crowns
Authorization is required for fixed dentures (that are cost-effective) for people who are unable to use removable dentures because of their medical condition.
Replacement of damaged fixed denture for individuals who are unable to use a removable denture due to a medical condition requires authorization.
Requests for authorization for fixed denture must be submitted with the following documentation:
- Medical and dental history which supports the medical necessity
- The member’s mental/physical condition including ICD-10-CM and DSM III-R diagnoses that cause the member’s inability to use a removable denture
- An explanation of the reason the member is unable to use a removable denture
- Radiographs of the current dental condition. Include copies (not originals) of X-rays.
- The specific treatment plan and the long-range prognosis for the remaining dentition
Codes
- D6545 – Retainer – cast metal
- D6548 – Retainer – porcelain/ceramic
- D6624 – Inlay – titanium
- D6634 – Onlay – titanium
- D6710 – Crown – indirect resin-based composite
- D6720 – Crown – resin with high noble metal
- D6721 – Crown – resin with predominantly base metal
- D6722 – Crown – resin with noble metal
- D6740 – Crown – porcelain/ceramic
- D6750 – Crown – porcelain fused to high noble metal
- D6751 – Crown – porcelain fused to predominantly base metal
- D6752 – Crown – porcelain fused to noble metal
- D6753 – Retainer crown – porcelain fused to titanium and titanium alloys
- D6780 – Crown – 3/4 cast high noble metal
- D6781 – Crown – 3/4 cast predominately based metal
- D6782 – Crown – 3/4 cast noble metal
- D6783 – Crown – 3/4 porcelain/ceramic
- D6784 – Retainer crown 3/4 – titanium and titanium alloys
- D6790 – Crown – full cast high noble metal
- D6791 – Crown – full cast predominantly base metal
- D6792 – Crown – full cast noble metal
- D6793 – Crown – provisional retainer crown
- D6794 – Crown – titanium
- D6920 – Connector bar
- D6940 – Stress breaker
- D6950 – Precision attachment
- D6985 – Pediatric partial denture, fixed
Oral Surgery
Authorization is always required for the codes listed in the Oral Surgery Codes Requiring Authorization section.
PrimeWest Health utilizes American Dental Association (ADA) code definitions for all dental procedure Service Authorization reviews, including oral surgery.
PrimeWest Health has formally adopted the American Association of Oral and Maxillofacial Surgery (AAOMS) Parameters of Care guidelines as the generally accepted clinical standards for the practice of oral and maxillofacial surgery
The routine prophylactic removal of third molars and other impacted teeth is not a covered service. Third molar and impacted teeth extractions must have symptoms and show evidence of pathology to substantiate the medical necessity for removal.
A referring provider must release the member’s health record (MN Stat. sec. 144.293) to another provider regardless of the status of the member’s account (MN Rules part 3100.9600). Rendering providers are responsible for working with the referring provider to obtain all needed documentation to request an authorization for a PrimeWest Health-covered service.
Extractions
Extractions of impacted teeth must meet the specifications of utilization criteria.
Third molars and other impacted teeth must be symptomatic and show evidence of active pathology.
To request a Service Authorization for the removal of an impacted tooth, the following dental history, case information, and documentation must be submitted for each tooth to be extracted:
Impacted Teeth
Requests for authorization must include per tooth documentation of evidence of pathology along with documentation that supports the medical necessity for each tooth’s removal, such as the following:
- Presence of severe pain or swelling with tooth number or quadrant noted
- Documented recurrent episodes of pericoronitis with tooth number or quadrant noted
- An episode of cellulitis, with tooth number or quadrant noted
- An episode of abscess formation or untreatable pulpal or periapical pathology with tooth number noted
- Active current periodontal disease due to the position of the third molar and its association with the second molar. Designate per tooth number in the request.
- External resorption of the third molar or of the second molar where this would reasonably appear to be caused by the third molar. Indicate tooth number(s).
- A non-restorable carious lesion on a partially erupted third molar or a carious lesion on the distal of the second molar due to the position of the third molar, including tooth number(s)
- A pathological condition such as a dentigerous cyst or other related pathology. Indicate with tooth number or quadrant
Submit authorization requests with the following documentation:
- Medical, dental, and behavioral histories that support medical necessity for the member
- Additional pertinent information
- Oral and Maxillofacial Surgery Medical Necessity Questionnaire on the medical review agent website
- Documentation of pathology for each tooth to be extracted, by tooth number
- Periodontal charting (when applicable) of the teeth recommended for extraction
- Copies of current radiographs with diagnostic value and chart documentation for each tooth to be extracted. X-rays must be mounted (when applicable), and be labelled with patient name and the date of X-ray exposure. Do not submit original X-rays; they could be lost and compromise the member’s care.
Omission of a portion of the above documentation will result in a Service Authorization denial.
Documentation should always be supplied by the provider who will be performing the extraction. Documentation of clinical observations made by the provider in the member’s chart notes during the member’s examination may be included. The requirements listed above need to be specific to the tooth/area affected and should be clearly identified.
To meet the documentation requirements, providers can submit clinical findings, the diagnosis, and a treatment plan along with a summary letter stating the member’s chief complaint. Letters submitted with this information should be signed by the provider, not office staff.
PrimeWest Health will deny any and all Service Authorization requests for oral surgery that do not meet the following section of the AAOMS guidelines:
"The OMS [Oral and Maxillofacial Surgeon] is responsible for an initial history and physical evaluation necessary to determine the risk factors associated with management of each patient. In some circumstances, the patient’s primary care physician or general dentist may perform the history and physical examination, but it is the responsibility of the OMS to review such information and ascertain whether it is complete to his/her level of satisfaction or whether further assessment is indicated based on the specific patient and planned procedure."
The primary services/procedures must be covered services under PrimeWest Health for ancillary services to be covered. If the primary procedure is not a covered service, regardless of the complexity or difficulty, coverage of services such as the administration of anesthesia, diagnostic X-rays, and other related procedures will not be covered.
Dentists and oral surgeons who perform medical procedures must follow the practitioner and general authorization guidelines for exams, consultation, radiology, surgery, anesthesia, and laboratory services.
A coronectomy instead of complete extraction can be performed if the following criteria are met:
- The tooth must demonstrate pathology or medical necessity with high risk of inferior alveolar nerve (IAN) injury to justify coronectomy. The anatomy must be amenable to complete removal of enamel and reduction of the remaining tooth structure to 3mm below the level of the bone.
- The tooth must not be mobile
- The tooth must not be actively infected (chronic periodontitis on the adjacent second molar is acceptable)
- The tooth must not have a cyst or tumor associated with it
- The tooth must not have decay into the pulp
Authorization requests for coronectomy must include a screen shot of the pertinent sections only of the CBCT. These must be of diagnostic quality with respect to the tooth or teeth being requested for authorization and clearly labeled according to Board of Dentistry protocol.
Submit authorization requests with the following documentation:
- Medical, dental, and behavioral histories that support medical necessity for the member
- Additional pertinent information
- Documentation of pathology for each tooth to be extracted, by tooth number
- Periodontal charting (when applicable) of the teeth recommended for extraction
- Current radiographs and/or CBCT with diagnostic value and chart documentation for each tooth to be extracted
X-rays and other images must be mounted (when applicable) and be labeled with the member's name and the date of X-ray exposure. Do not submit original X-rays as they could be lost and compromise the member’s care.
Oral Surgery Codes Requiring Authorization (not an all-inclusive list)
- D7220 – Removal of impacted tooth – soft tissue
- D7230 – Removal of impacted tooth – partial bony
- D7240 – Removal of impacted tooth – completely bony
- D7241 – Removal of impacted tooth – completely bony, with unusual surgical complications
- D7251 – Coronectomy – intentional partial tooth removal
- D7272 – Tooth transplantation
- D7290 – Surgical repositioning of teeth
- D7291 – Transseptal fiberotomy
- D7490 – Radical resection of maxilla or mandible
- D7953 – Bone replacement graft
Temporomandibular Joint Disorder (TMD)
Authorization is always required.
- D7899 – Unlisted TMD therapy
- D7880 – Occlusal orthotic appliance
- 41899 – Unlisted procedure, dentoalveolar structures
Orthodontic
Orthodontic treatment that meets the specifications of utilization criteria .
Authorization is always required.
Combined orthognathic surgery and orthodontia coverage guidelines
If orthodontics are necessary in preparation for orthognathic surgery, the orthognathic surgery must be approved by PrimeWest Health first. When submitting a Service Authorization request for a combined orthognathic surgery and orthodontia treatment plan, provide PrimeWest Health with details of the proposed combined orthognathic surgical/orthodontic treatment at that time. If a PrimeWest Health member was approved for orthodontia or orthognathic surgical treatment of a skeletal/dental malocclusion from a previous health plan, notify PrimeWest Health of this when the member has transitioned to PrimeWest Health coverage. Regardless of the member’s state of treatment, there must either be a previous approval in place for the surgery or you must obtain authorization for the surgery from PrimeWest Health in order for the procedure to be performed and covered by PrimeWest Health.
Criteria
The need for orthodontic treatment must be exhibited by medical functional impairment (see definition below). Patients with dental or orthodontic needs only will not be approved for orthodontic treatment by PrimeWest Health.
Comprehensive orthodontic treatment is considered medically necessary when adequate corrective treatment for developing an adequate biting/chewing relationship is not achievable with less extensive means and one of the following criteria is met:
- Overjet greater than 9 mm
- Reverse overjet greater than 3.5 mm
- Anterior or posterior cross bite, or both, of three or more teeth per arch
- Lateral or anterior open bite 2 mm or more; of four or more teeth per arch
- Impinging overbite with evidence of occlusal contact into the opposing soft tissue
- Impactions where eruption is impeded by extraction is not indicated (excluding third molars)
- Jaws or dentition, or both, which are profoundly affected by a congenital or developmental disorder (craniofacial anomalies), trauma, or pathology
- Congenitally missing teeth (excluding third molars) of at least one tooth per quadrant
- Crowding or spacing of 10mm or more, in either the maxillary or mandibular arch (excluding third molars)
- Other conditions as deemed medically necessary (must include narrative)
Orthodontic care usually requires lengthy treatment. It is recommended that the provider discuss the expected eligibility period with the family and the county human services agency before initiating treatment. This will clarify the eligibility policies and help reduce denial of payment, due to subsequent ineligibility. A member’s eligibility can terminate or may go from FFS to MCO on a month-to-month basis.
Providers are encouraged to consult with parents/guardians regarding noncompliance and disregard for instructions. Treatment may be terminated and all appliances removed until a later time when the child is more mature and can follow instructions. Compliance is critical for a successful orthodontic outcome. Noncompliance with orthodontic treatment can negatively affect the child by exacerbating oral disease.
Submit requests for orthodontic authorization with the following documentation:
- ADA dental claim form or supporting clinical documentation identifying the noted qualifying criteria and associated tooth numbers, or measurements as required
- Medical, dental, and behavioral histories that support medical necessity for the member
- Additional pertinent information
- Specific treatment plan and appliances (enter appropriate procedure code)
- Five intraoral photographs labelled with the member name and date taken; upper and lower occlusal; prints or mounted slides are acceptable; include profile photos
- Appropriate radiographs (panoramic or full mouth and cephalometric) labelled with patient name and date of exposure.
Codes
- D8010 – Limited orthodontic treatment of primary dentition
- D8020 – Limited orthodontic treatment of transitional dentition
- D8030 – Limited orthodontic treatment of adolescent dentition
- D8040 – Limited orthodontic treatment of adult dentition
- D8070 – Comprehensive orthodontic treatment of transitional dentition
- D8080 – Comprehensive orthodontic treatment of adolescent dentition
- D8090 – Comprehensive orthodontic treatment of adult dentition
- D8091 – Comprehensive orthodontic treatment with orthognathic surgery
- D8210 – Removable appliance therapy
- D8220 – Fixed appliance therapy
- D8670 – Periodic orthodontic treatment visit
- D8671 – Periodic orthodontic treatment visit associated with orthognathic surgery
- D8680 – Orthodontic retention
- D8681 – Removable orthodontic retainer adjustment
- D8696 – Repair of orthodontic appliance – maxillary
- D8697 – Repair of orthodontic appliance – mandibular
- D8698 – Re-cement or re-bond fixed retainer – maxillary
- D8699 – Re-cement or re-bond fixed retainer – mandibular
- D8701 – Repair of fixed retainer, includes reattachment – maxillary
- D8702 – Repair of fixed retainer, includes reattachment – mandibular
- D8703 – Replacement of lost or broken retainer – maxillary
- D8704 – Replacement of lost or broken retainer – mandibular
- D8999 – Unspecified orthodontic procedure
Other Dental Services that Require Service Authorization
Submit requests for authorization with the following dental history, case information, and documentation:
- Medical and dental history that supports the medical necessity.
- Copies of current radiographs that show the current dental condition.
- Complete treatment plan and long-range prognosis for the remaining dentition.
Codes
- D9941 – Fabrication of athletic mouth guard
- D9952 – Occlusal adjustment, complete
- D9971 – Odontoplasty, includes removal of enamel projections
- D9972 – External bleaching – per arch
- D9973 – External bleaching – per tooth
- D9974 – Internal bleaching – per tooth
- D9999 – Unspecified adjunctive procedure, by report
Orthodontic Billing
Use D8660 pre-orthodontic treatment visit to report orthodontic full case study.
The retention phase of orthodontic treatment is a component of the comprehensive orthodontic care for which the provider is reimbursed. The type of retention is a choice made by the provider. Do not bill the member.
Post-orthodontic treatment records are included in the orthodontic services authorized. Providers should not bill PrimeWest Health for post-orthodontic cephalometric films.
For comprehensive orthodontic treatment:
- Use D8999 for initial banding and write “initial banding” in the narrative
- Bill adjustments utilizing the appropriate comprehensive code (D8070, D8080, or D8090)
Replacement and/or re-cementing of one or two brackets due to reasonable wear and tear is considered a part of the total orthodontic treatment. Re-cementing of brackets due to a failure of the patient to comply with provider instructions is a non-covered service, and the provider may bill the member for the cost. Since re-cementation of brackets is not a covered service, the provider is not required to submit charges to PrimeWest Health.
The retention phase of orthodontic treatment is a component of the total orthodontic care for which the provider is reimbursed. The type of retention is a choice made by the provider. Do not bill the member.
Authorization Requirements for PrimeWest Health Members with Third Party Liability (TPL) Insurance
Billing PrimeWest Health depends on the authorization type received.
| If the PrimeWest Health authorization approves an initial appliance placement and subsequent monthly adjustments | Bill using the following instructions: If the TPL/other insurance pays an initial down payment and subsequent payments over the course of the treatment (monthly, quarterly, semi-annual, or annual payments):
If the TPL/other insurance pays over the entire course of the orthodontic treatment (monthly, quarterly, semi-annual, annual, or lump sum payments):
|
| If the PrimeWest Health authorization approves only monthly adjustments | Bill using the following instructions: If the TPL/other insurance makes payments over the course of the treatment:
Use one of the following two examples to calculate the prorated payment amounts:
|
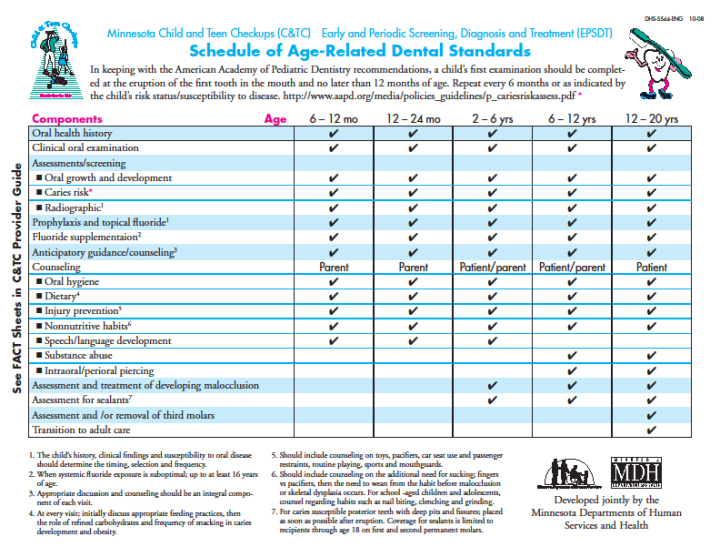
Dental Periodicity Schedule
As required by the Centers for Medicare & Medicaid Services (CMS), the Schedule of Age-Related Dental Standards (DHS-5544-ENG) was developed. This schedule, which is in keeping with recommendations of the American Academy of Pediatric Dentistry, must be utilized by both primary care and dental providers.
Primary care providers should perform an oral exam as part of the physical exam at every C&TC screening. Early access to high-risk children provides opportunities for primary care providers to partner with dental providers to ensure that children receive dental care. A collaborative effort between primary care and dental providers is essential.
Primary care providers should complete caries risk assessments, anticipatory guidance, and referrals to dentists. Other components of the Schedule of Age-Related Dental Standards (DHS-5544-ENG) are elements that should be completed as part of C&TC screenings and as part of a dental visit. A child’s first oral evaluation by a dentist should be completed at the time of the eruption of the first tooth in the mouth or no later than 12 months of age.
Dental Supplemental Benefits for PrimeWest Senior Health Complete and Prime Health Complete Members
PrimeWest Health Senior Health Complete (HMO SNP) and Prime Health Complete (HMO SNP) members may be eligible for additional supplemental benefits for dental services. Review the Supplemental Benefits guide for more information.
Members with the following division numbers are eligible for the denture supplemental benefit:
- MSHO001-0004
- MSHO001-0005
- MSHO001-0006
- MSHO001-0007
- MSHO001-0008
One additional replacement set of dentures (one maxillary and one mandibular) every six years.
Authorization is always required.
Submit a completed Denture Replacement Request Form.
Codes
- D5110 – complete denture – maxillary
- D5120 – complete denture – mandibular
- D5130 – immediate denture – maxillary
- D5140 – immediate denture – mandibular
- D5211 – maxillary partial denture, resin base
- D5212 – mandibular partial denture, resin base
- D5213 – maxillary partial denture, cast metal
- D5214 – mandibular partial denture, cast metal
- D5225 – maxillary partial denture, flexible base
- D5226 – mandibular partial denture, flexible base
- D5221 – immediate maxillary partial denture, resin base
- D5222 – immediate mandibular partial denture, resin base
- D5223 – immediate maxillary partial denture, cast metal
- D5224 – immediate mandibular partial denture, cast metal
- D5227 – immediate maxillary partial denture, flexible base
- D5228 – immediate mandibular partial denture, cast metal
- D5820 – interim partial denture (maxillary)
- D5821 – interim partial dentures (mandibular)
PrimeWest Senior Health Complete and Prime Health Complete members with the following division numbers are eligible for the crown supplemental benefit:
- MSHO001-0004
- MSHO001-0005
- MSHO001-0006
- MSHO001-0007
- MSHO001-0008
- SNBC01-008
- SNBC01-009
- SNBC01-0010
- SNBC01-0011
- SNBC01-0012
- SNBC01-0013
One porcelain crown per calendar year up to a limit of $1,500.
Authorization is always required.
Submit the following with a Service Authorization request:
- Recent diagnostic periapical X-ray (not a panoramic) showing the affected tooth to be crowned
- Supporting statement regarding the clinical observations and rationale for treatment signed by the attending provider
- Statement indicating whether the crown is occluding with a denture, a removable prosthesis (RPD), or natural dentition
- Clinical photos that show the appearance of the tooth that has a condition (such as cracked tooth syndrome) that cannot be diagnosed by a periapical radiograph alone
- Periodontal probings and evidence of periodontal therapy if the tooth appears to have bone loss
- Indication of tooth numbers to be extracted or that have already been extracted
Crowns may be approved for dental necessity when a tooth has been compromised by any of the following:
- Breakage (accidental or otherwise) of part of the tooth or a previous large filling, rendering the tooth incapable of being restored adequately and successfully by any other conservative filling material/technique, such as alloy or composite
- Treatment with a root canal filling when the tooth is a posterior tooth or the clinical crown is composed of over 75 percent filling material
- Cracked tooth syndrome, where circumferential coverage is required to adequately restore the tooth
- Replacement of an existing crown due to fracture of porcelain or recurrent caries
The tooth to be crowned should have at least a one-to-one crown-to-root ratio.
Coverage exclusions for porcelain crowns include, but are not limited to, the following:
- Crowns for cosmetic reasons
- Crowns to reestablish or treat occlusion (such as decreased vertical dimension), TMD, grinding, or erosion
- Crowns submitted for enamel cracks, abfractions, pitting, tetracycline staining, fluorosis, etc.
Codes
- D2740 – crown – porcelain/ceramic substrate
- D2750 – crown – porcelain fused to high noble metal
Code not included
- D2950 – core buildup
PW_11-18_430
Updated_10/13/2025

